I was honored to give a talk at Society for Hospital Medicine Converge 2023. The talk discussed our successful collaboration with UCSF that demonstrated the feasibility and utility of an artificial intelligence-powered computer vision camera to monitor patients at high risk of delirium. We were excited by the ability to capture activity patterns that are highly relevant to delirium (e.g. rest/wake disruption, hyper/hypoactivity) without wearable devices. We also were excited by the ability to capture new data streams relevant to delirium care (e.g. bedside activity by staff & visitors, room light levels throughout the day).
The need for new monitoring technologies for delirium
Delirium is an acute and fluctuating disturbance of consciousness and cognition, characterized by confusion, disorientation, and often accompanied by hallucinations or delusions. Also known as acute brain failure, it impacts many (if not most) older adults admitted to the hospital. It is expensive, decreases the value of care, and leads to worse outcomes. Concerningly, the impact of delirium follows a patient home with higher risks for impaired cognition and even death in the months after discharge.
Despite the need, monitoring for delirium remains largely manual and intermittent, even though it can acutely worsen and characteristically wax and wane. Additionally, there are few approaches for monitoring the care environment, even though the care environment is a major factor in preventing and treating delirium. Visual monitoring methods are promising because they can capture patient activity patterns that are characteristic of delirium as well as key factors in the hospital environment.
AI computer vision as a new paradigm for delirium monitoring
Computer vision enables machines to interpret and understand visual data from the world around us. This interpretation is a kind of artificial intelligence that, up until recently, was only possible by humans. This intelligence has been powered by advances in machine learning methods such as deep learning and convolutional neural networks.
As more cameras make their way into hospital rooms for telemedicne, the opportunity arises to make these cameras “smart” using computer vision technologies. For delirium, these smart cameras may complement existing monitoring approaches since they can continuously monitor both patient motion and room environment. With this in mind, we pursued our collaboration with UCSF.
Computer vision and delirium study details
We ran a feasibility pilot study on the Acute Care for Elders (ACE) unit at UCSF. It was an IRB-approved study where patient at risk for delirium (but not delirious) were prospectively consented for enrollment. We used a color + nigh vision camera that streamed video to an encrypted hard drive. After recording was complete (typically a few days), the video was run through AI-enabled CV algorithms to generate time-series data streams. De-identified videos were made by full-frame blurring. Additionally, image-based readouts were generated.
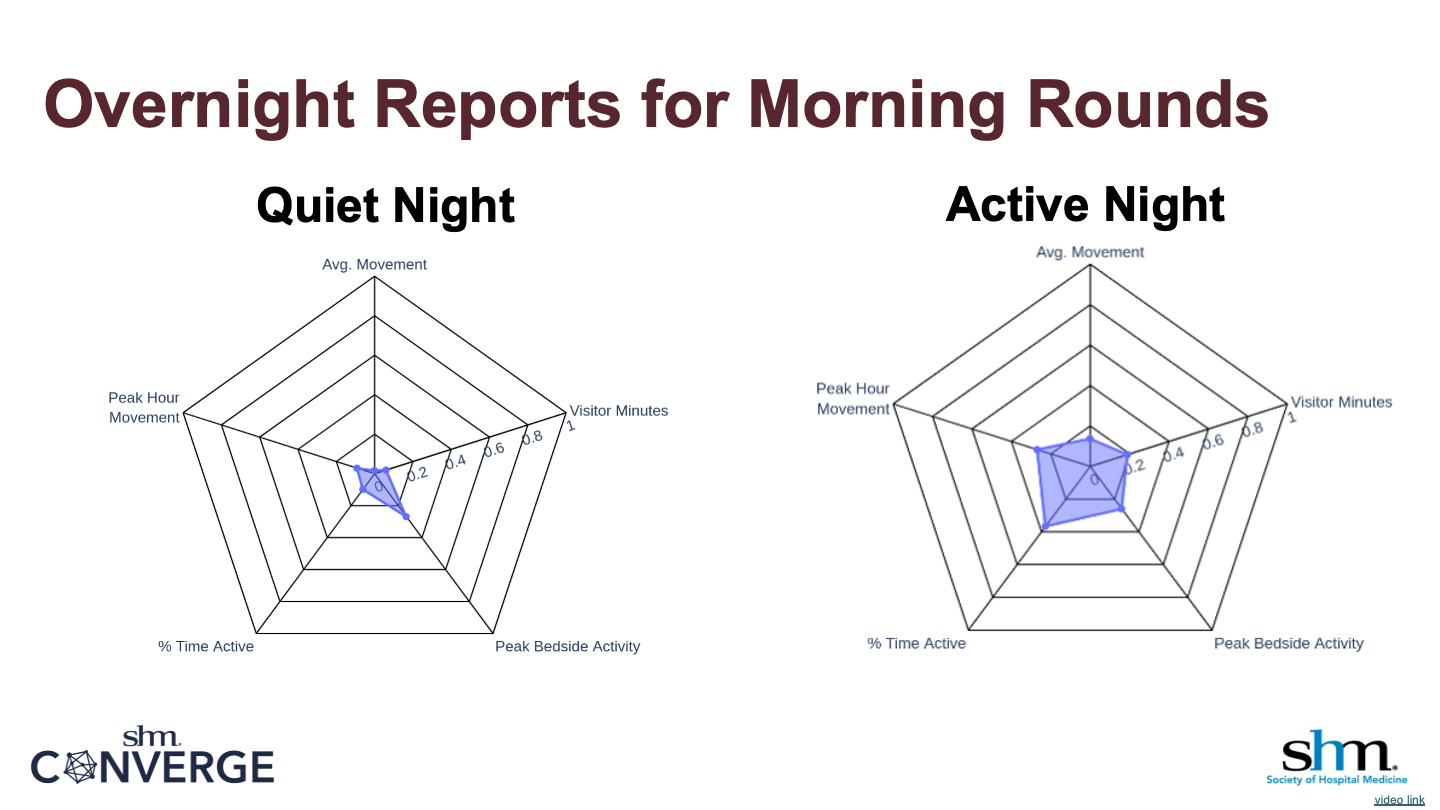
The results, we believe, were convincing in showing feasibility, especially given the importance of motion in delirium. As an example, not only did itself video capture significant nighttime activity in patients, but this activity was summarized in AI computer vision data. These data can be displayed in easy to digest overnight reports that summarize patient activity along three dimensions and care environment along two dimensions.
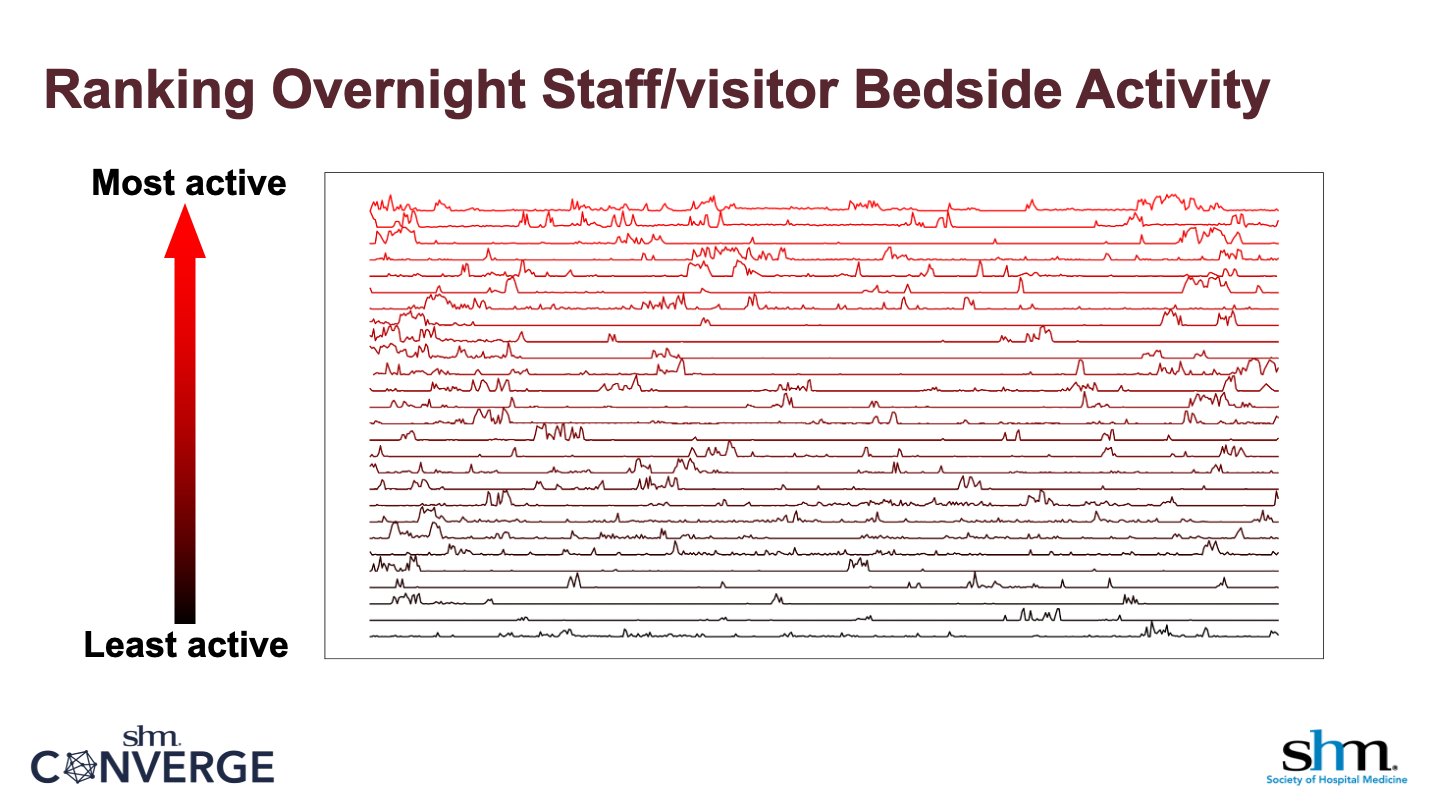
Using histogram analysis, we generated percentile cutoffs for patient activity and bedside attention by staff and visitors (a proxy measure for patient acuity). To demonstrate the potential of generating these normative statistics, we sorted all complete nighttime periods from least to most busy in terms of bedside attention. Clinical attention is a strong signal for not only clinical acuity but also disposition. Higher levels of attention may mean a higher level of care is needed (e.g. stepdown unit); lower levels of attention may mean that the patient can go to a lower level of care (or even home).
Closing thoughts
We note that, on one hand, none of the patients enrolled in the study were clinically diagnosed with delirium using Nu-DESC criteria. On the other hand, the ability to have continuous, quantitative data on rest/wake cycles and hypo/hyperactivity may allow the many components of delirium to be “unbundled” in a way that is clinically actionable. It is important to identify extremes of activity and sleep disruption in patients at-risk for delirium, regardless of Nu-DESC or CAM status. Once identified, AI computer vision data provides a basis for tracking clinical clinical progress of individual patients and efficacy of QI efforts to improve these components.
The talk was “Feasibility testing and clinical utility of a continuous artificial intelligence-powered computer vision monitoring system for hospitalized patients at risk of delirium”
LookDeep authors
Paolo G. Gabriel, PhD; Laura Urbisci, PhD; Tyler Troy, PhD; Tom Hata, PhD; Narinder Singh, MBA, MTM; Michael A. Choma, MD, PhD
UCSF authors
Steven Yim, BS; James D. Harrison, PhD; Stephanie E. Rogers, MD; Sasha Binford, PhD, MS, RN, PHN, AGCNS-BC