


Best Practices Guide: Enhancing Rural Hospital Care with AI-Powered Virtual Monitoring
Overview
Rural hospitals operate under significant constraints with limited staffing and resources. AI-powered virtual monitoring leverages computer vision technology to extend care capacity. Hospitals adopting these platforms have achieved impressive results: 70-90% reductions in patient falls among monitored populations, with coverage expanding from just 5-10% to over 95% of high-risk patients.
The new Rural Health Transformation Fund provides funding opportunities for rural facilities to implement such technologies.
Starting with Fall Prevention
Fall prevention serves as the foundation for broader safety programs. Three core elements enable success:
- Leadership and buy-in across levels — Programs require commitment from both administration and frontline staff
- Simplicity — Technology must function reliably without requiring clinical teams to become IT specialists
- Technology as a multiplier — Systems should expand capacity, enabling one observer to monitor dozens of patients
Leadership and Buy-In
Personal experiences drive adoption. One chief nursing officer discovered her own mother wandering unsupervised, highlighting monitoring gaps. A caregiver noted, “I made sure my mom came here because I knew someone would be watching.” These stories transform technology adoption into sustained institutional commitment.
Simplified, Scalable Technology
Rural facilities frequently struggle with complex telehealth systems and unreliable equipment. While vendors claim 99.9% uptime, last-mile connectivity issues erode trust. Bridging the gap between technical specifications and actual clinical experience is essential for implementation success.
Technology as Capacity Multiplier
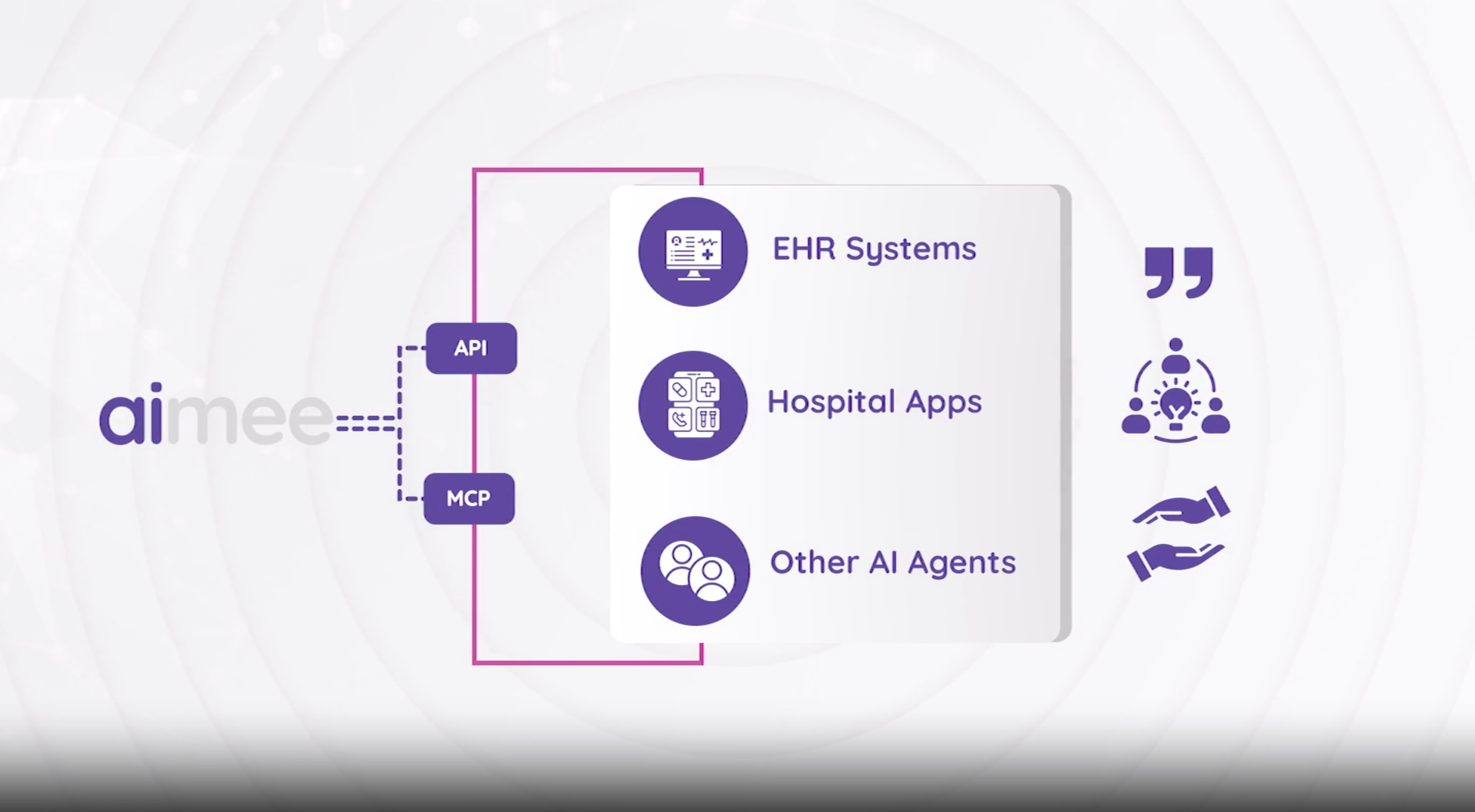
AI-powered monitoring represents the first technology capable of continuous visual and auditory observation in patient rooms. This enables one staff member to oversee all high-risk patients rather than a select few.
Research indicates rural hospitals adopt AI at lower rates than urban counterparts, yet their constrained resources mean AI delivers greater immediate impact. When technology extends nursing attention across dozens of patients, outcomes transform in settings where staff already manage multiple roles.
Beyond Falls: Expanded Applications
The same monitoring systems support additional clinical capabilities:
- Proactive pressure injury detection
- Alerts for mobility changes
- Workplace violence prevention
- Patient companions for routine requests (meal discussions)
One physician noted ordering telemetry simply to ensure vulnerable patients received attention. Continuous monitoring now provides this vigilance by design without additional equipment or workarounds.
Conclusion
Rural hospitals need AI solutions designed for their specific context — smaller settings where individuals contribute across multiple functions. Rather than adding dashboards, effective technology works bedside with staff, supporting direct patient care. When designed appropriately, AI extends nursing capacity, giving clinicians the support needed to deliver collaborative, patient-centered care.
Related Articles
Continue exploring insights on similar topics.
The Chair Problem – What Every Nurse Should Know About Seated Fall Risk

New Research: Exposure-Normalized Bed and Chair Fall Rates via Continuous AI Monitoring
