Accelerating Your AI Future with the Video Dial Tone — or Slowly Killing It Without One

Watch: The Video Dial Tone — 90 seconds
By Narinder Singh, CEO — LookDeep Health
Why every hospital making video infrastructure decisions today should demand openness — and what a hundred years of telephony teaches us about getting it right.
When Alexander Graham Bell patented the telephone in 1876, telephony began as a proprietary island. Phones could only connect within the same company’s network. If your town had two competing telephone companies, you might literally need two phones on your desk, one for each.
As the network grew, it became something bigger than a product: it became infrastructure. And whoever controlled that infrastructure controlled the future. For much of the twentieth century, the dominant model was simple: one company owned the lines, the switches, the devices, the standards — and the rules. It wasn’t just hard to attach your own device to the network; it was illegal. Innovators resorted to absurd workarounds — acoustic couplers, literally holding a speaker to a handset — just to avoid “touching” the system directly.
Then in 1968, the Carterfone decision cracked the logic of captivity. If a device doesn’t harm the network, it should be allowed to connect. That one principle opened the door to a world where the network wasn’t one vendor’s product. It was a shared platform.
And that’s what the dial tone came to represent: pick up the receiver, hear that steady tone, and know the entire network is available to you. Open. Connected. Full of possibility.
Hospital video today is back at the beginning of that story.
The first generation of virtual care solutions were built with good intentions: ship something integrated, reliable, and turnkey. Proprietary cameras. Proprietary software. Proprietary AI. Bundled into a single stack that “just worked.” For early adopters, that integration felt like a feature.
But somewhere along the way, integration quietly turned into control.
Switching costs became the business model. Hospitals that installed one vendor’s hardware discovered they couldn’t run another vendor’s software — or even keep their cameras if they changed platforms. The infrastructure became a lever. Not a foundation.
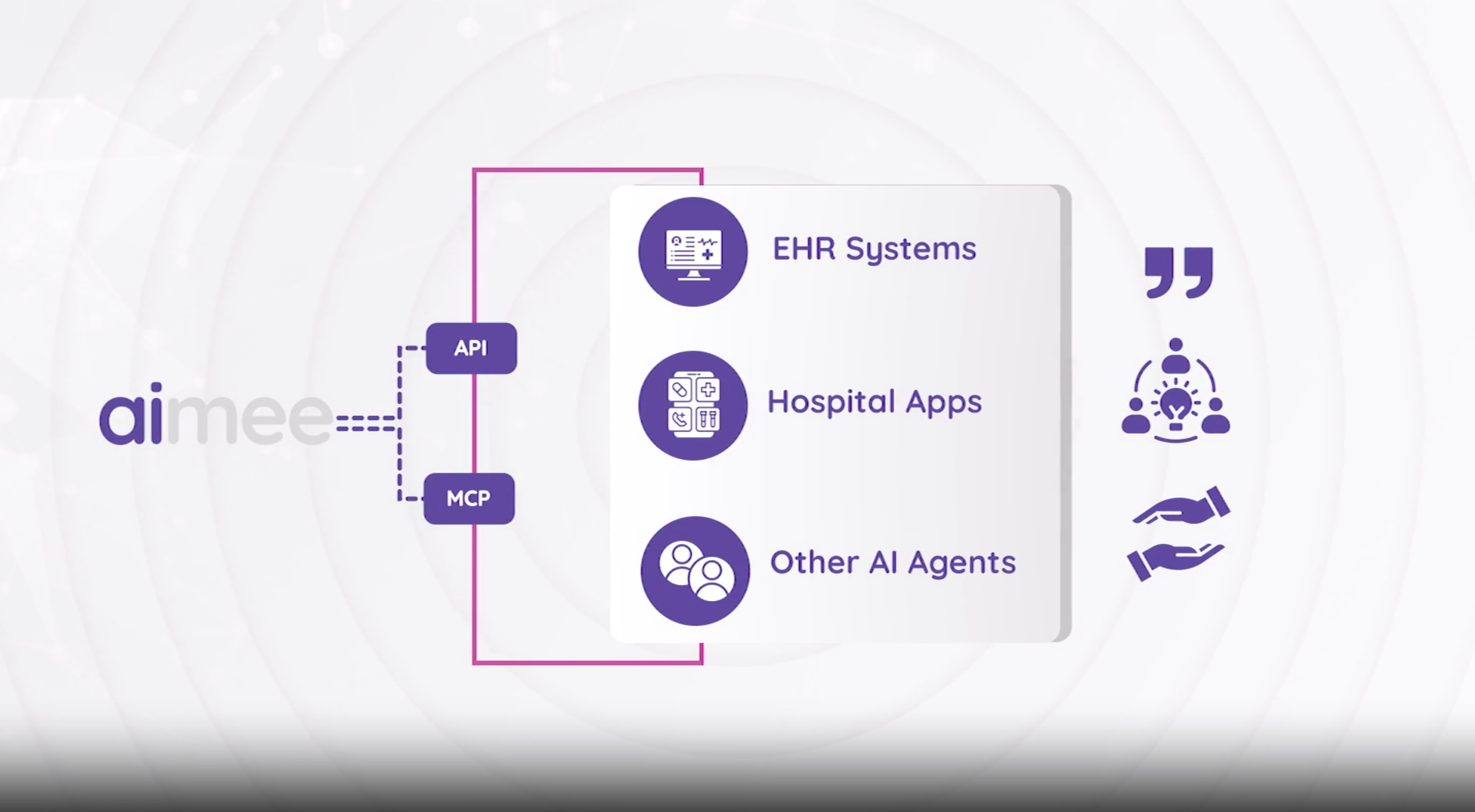
That matters now more than ever, because in-room video and audio are becoming the foundational infrastructure for the next era of care. Virtual nursing. AI-powered patient safety. Ambient documentation. Agentic AI at the bedside. The next decade of clinical innovation will run on that stream of sight and sound. Yet much of the market still sells it like a closed appliance: proprietary hardware fused to proprietary software.
Want to try a better AI model next year? A better workflow? A better platform? You may have to rip out your cameras. Your investment isn’t really yours.
Early computing pioneer Bill Joy once observed that no matter who you are, most of the smartest people work for someone else. That’s the case for open infrastructure in a single sentence. The best AI for hospital care won’t all come from one vendor. A closed stack bets your future on one company’s roadmap. An open foundation lets the entire ecosystem work for you.
We are far more certain about the future of in-room video over the next ten years than we are about what AI will create on top of it. That asymmetry is exactly why the infrastructure must be open.
The Video Dial Tone Commitment
So LookDeep is making a commitment we’re calling The Video Dial Tone: if you deploy our next-generation video infrastructure, it stays open and usable — period — even if you choose a different software platform later. Any AI. Any workflow. Any platform.
This isn’t a call for fragmentation. You can absolutely choose a single partner and an integrated solution — and many hospitals probably should. But you should not be captive to them. Future-proofing isn’t a feature request. It’s a design principle for infrastructure that matters.
This is how civilization has always made its best investments. Bridges, roads, power grids, fiber networks — the infrastructure is substantial, durable, and built to outlast whatever runs on it. The innovation on top is fast, competitive, and unpredictable. CEOs invest bigger in foundations they trust will survive change. Boards approve capital when they know the asset won’t be obsolete in five years. That confidence is what turns pilots into enterprise commitments.
And if you’ve already picked a solution partner and you’re deep into a rollout: demand this commitment for the rest of your deployment. A true partner shouldn’t fear it. There is no downside for hospitals — and no downside for vendors who genuinely believe their outcomes will win on merit. It’s the kind of clause you’ll never regret, and one day you may be deeply grateful you insisted on. Because the hospital that secures openness now won’t have to explain to a board three years from now why switching platforms means starting from zero.
We hope every vendor in this space follows this example. When infrastructure is open, the entire industry moves faster. Innovation competes on results instead of lock-in. And hospitals can finally invest in video the way they invest in buildings and networks — with confidence that the foundation will endure.
The Historical Lesson
It took nearly a hundred years to pry open the telephone network. And just as that openness finally arrived, the internet emerged — a network designed to be open from the very beginning — and turned telephony into just another application running on top. A century of fighting for interoperability, leapfrogged almost overnight by a platform that started with openness as a first principle.
The lesson is hard to miss: the phone industry spent a hundred years learning what the internet’s architects knew on day one. Build the foundation open, and you never have to fight that battle. Build it closed, and you eventually fight it anyway — you just lose the years in between.
The Urgent Need
Hospital video doesn’t have a hundred years.
Patients are scared at 2 a.m. and there is no one in the room. Families can’t be there when they want to be. Nurses are stretched to the point of breaking. A quiet change in breathing goes unnoticed until it isn’t quiet anymore. The AI that can help with all of this is coming fast — but only if it can reach the bedside as easily as software reaches a network.
The people inside our hospitals — patients and the staff who care for them — need relief now. Not after a decades-long fight for openness. Not after we untangle the lock-in we built today.
They need a dial tone.
This article was originally published on LinkedIn.
Related Articles
Continue exploring insights on similar topics.

Sibel Health and LookDeep Health Announce Strategic Partnership to Combine Continuous Vitals with Real-Time Bedside AI - Without Lock-In
LookDeep Health Platform Launches New Capabilities to Reduce Workplace Violence in Hospitals