
Your Fall Rates
Depend on a Variable
You've Never Been Able
to Measure – Until Now
New preprint from LookDeep Health –first-of-its-kind
research on chair falls in virtual observer programs


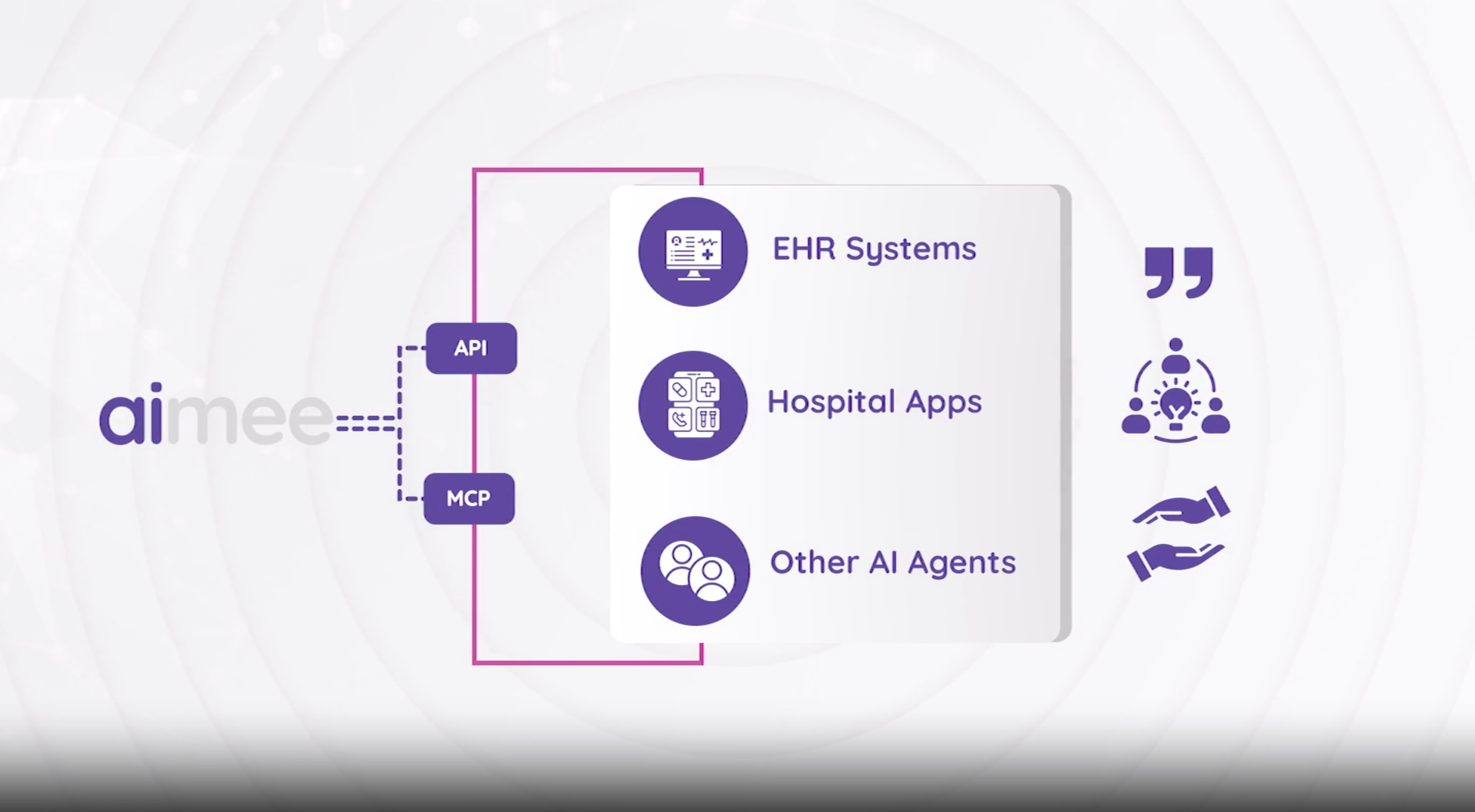
aimee — The First Clinical AI Assistant For Hospitals
aimee can see, hear, and talk to patients for doctors and nurses in the hospital. She monitors patients continuously, communicates in any language, and supports clinical teams across virtual sitting, nursing, and medicine — all from a single platform.
One Open Platform for All Virtual Needs
The LookDeep platform, powered by aimee, spans virtual nursing, virtual sitting, virtual medicine and more.

Virtual Observation
AI-powered fall prevention that continuously monitors patients, detects risk in real time, and alerts care teams — reducing falls by up to 90%.
Learn More →
Virtual Nursing
aimee handles admissions, rounding, discharge education, and documentation — giving bedside nurses back hours of their day.
Learn More →
Virtual Intelligence
Seamless consults, constant AI powered insights on your patients, integrated with leading devices and wearables.
Learn More →See What aimee Can Do
From preventing surgery cancellations to conducting pain assessments in any language, aimee handles real clinical workflows — autonomously.

Prevent Surgery Cancellations
aimee proactively monitors and prevents pre-surgical NPO violations

Purposeful Rounding Every Hour
Complete Patient Assessment Coverage (Purposeful Nurse Rounding)

Discharge Education - Wound Care
Delivers personalized wound care education and confirms understanding through guided review.

Patient Pain Assessment
aimee performs targeted pain evaluations as directed by clinical staff

Ordering Lunch (Spanish)
aimee helps a non english speaker who speaks Spanish as as secondary language order lunch.

Prevent Patient Leaving Room Alone
Prevents unsupervised patient wandering through proactive engagement

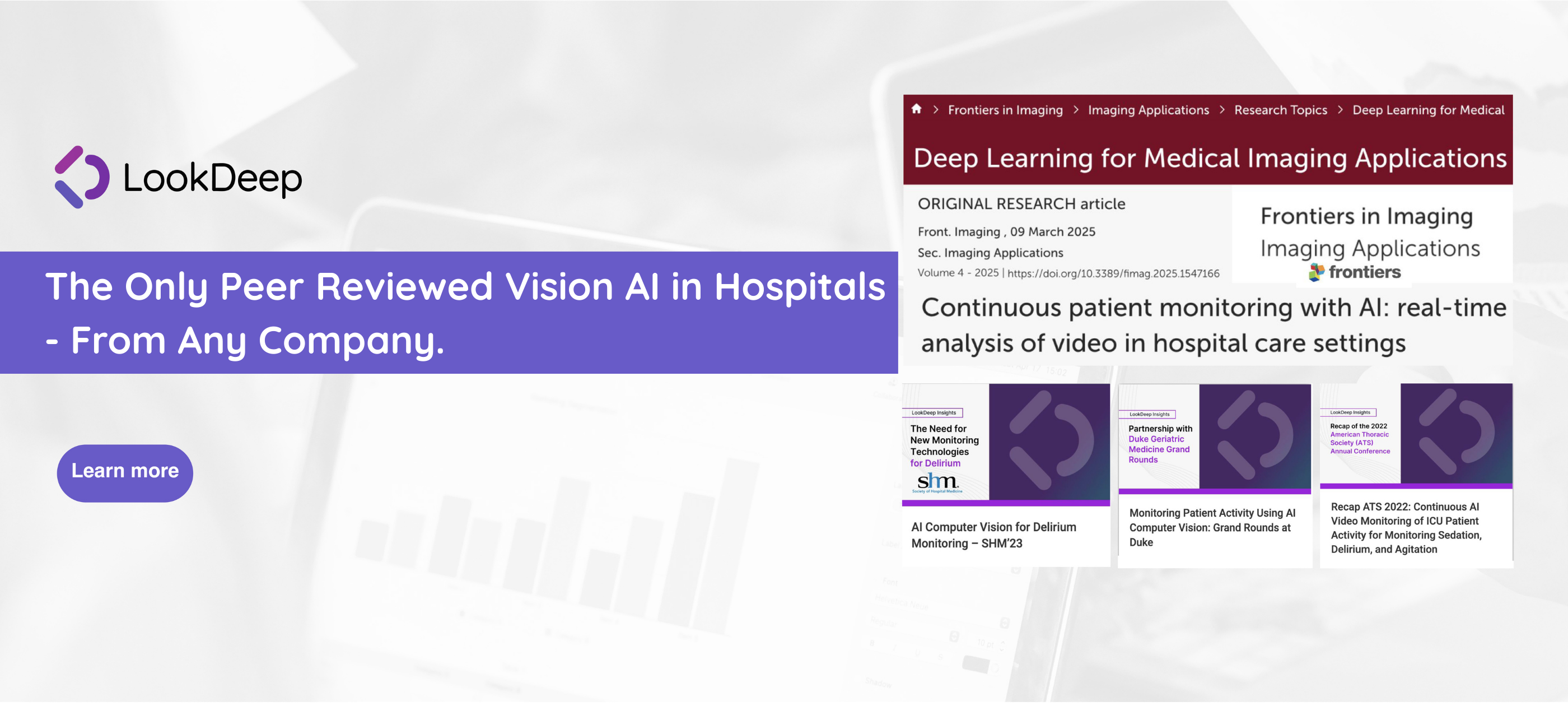
Peer-Reviewed Research. Real-World Results.
LookDeep is the only virtual care AI platform backed by independent, peer-reviewed clinical research. Our outcomes aren't marketing claims — they're published science.
- ✓ More views than 97% of all Frontiers articles
- ✓ In the top 25% of all research scored by Altmetric
Read the Research“Healthcare innovation typically advances in incremental steps, but aimee feels like a leap forward. Aimee has the potential of being an AI assistant that can understand the room, speak with empathy, and integrate into caregiver workflows, which is a transformative shift for hospitals.”
— Maria Russo, MBA, Chief Information Officer at OU Health
Latest Insights
AI drives an unprecedented pace of innovation for healthcare. LookDeep offers a strategic, highly technical and pragmatic view of the challenges facing hospitals.
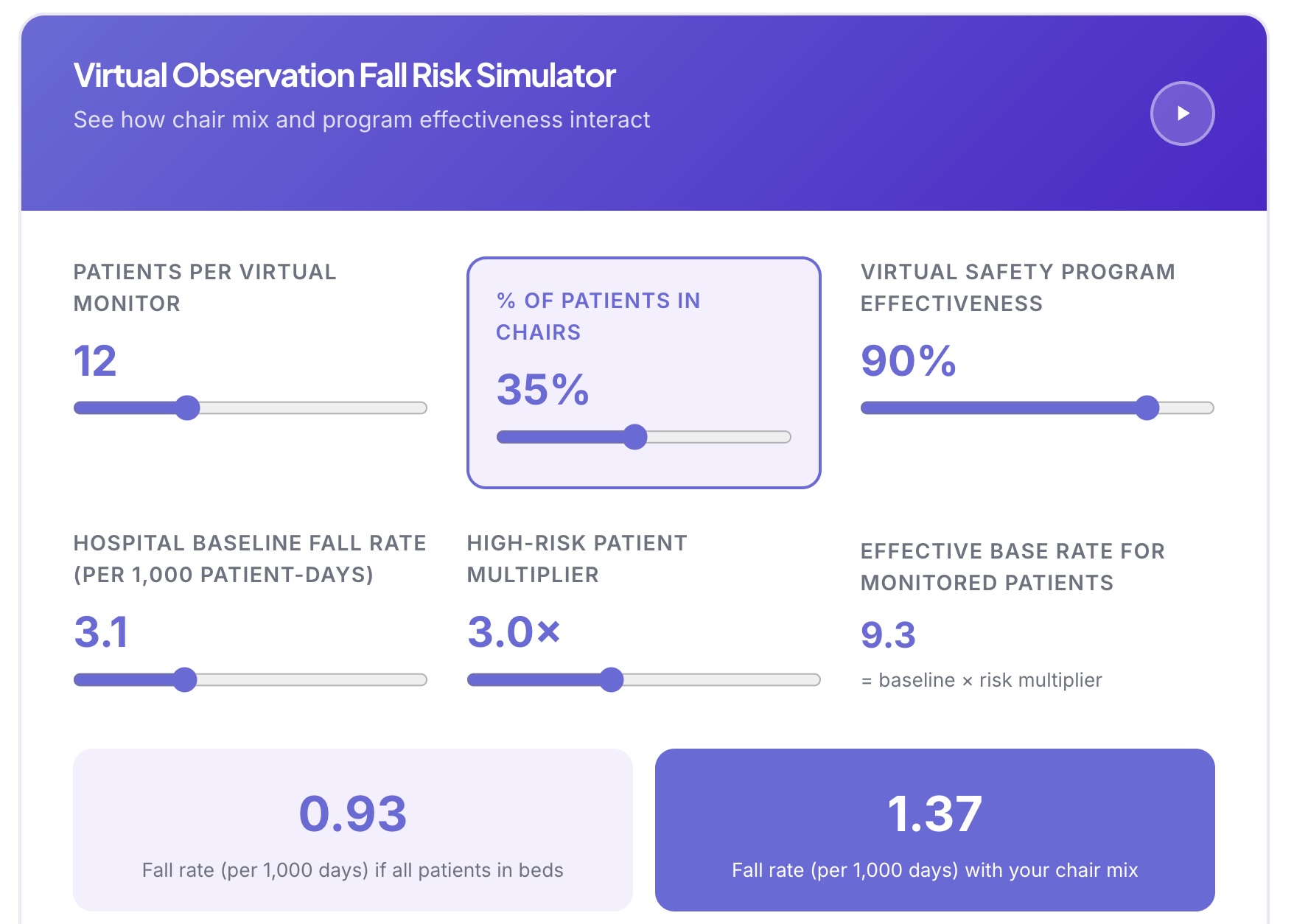
The Chair Problem – What Every Nurse Should Know About Seated Fall Risk
New Research: Exposure-Normalized Bed and Chair Fall Rates via Continuous AI Monitoring

Accelerating Your AI Future with the Video Dial Tone — or Slowly Killing It Without One

Sibel Health and LookDeep Health Announce Strategic Partnership to Combine Continuous Vitals with Real-Time Bedside AI - Without Lock-In
LookDeep Health Platform Launches New Capabilities to Reduce Workplace Violence in Hospitals